
Einführung
Few skin conditions frustrate dermatologists and patients alike as much as melasma—those stubborn brown or gray-brown patches that appear on the cheeks, forehead, and upper lip, often triggered or worsened by sun exposure. For sun-worshippers and beach lovers who enjoy outdoor activities, melasma can feel like an unfair punishment for doing what they love. This article explores how fractional laser strategies can help manage melasma effectively, combining clinical principles with practical advice for those who refuse to give up their time in the sun.
1. Understanding Melasma: The Sun Lover‘s Dilemma
1.1 What Exactly Is Melasma?
Melasma is a chronic, acquired hypermelanosis characterized by symmetric, irregularly bordered hyperpigmented patches on sun-exposed areas of the face. It most commonly affects the cheeks, forehead, upper lip, nose, and chin. Unlike temporary tanning or simple freckles, melasma involves deep-seated pigment deposits within both the epidermis and dermis. This explains why topical creams alone often fail to clear it completely.
1.2 The Sun Connection: Why UV Radiation Drives Melasma
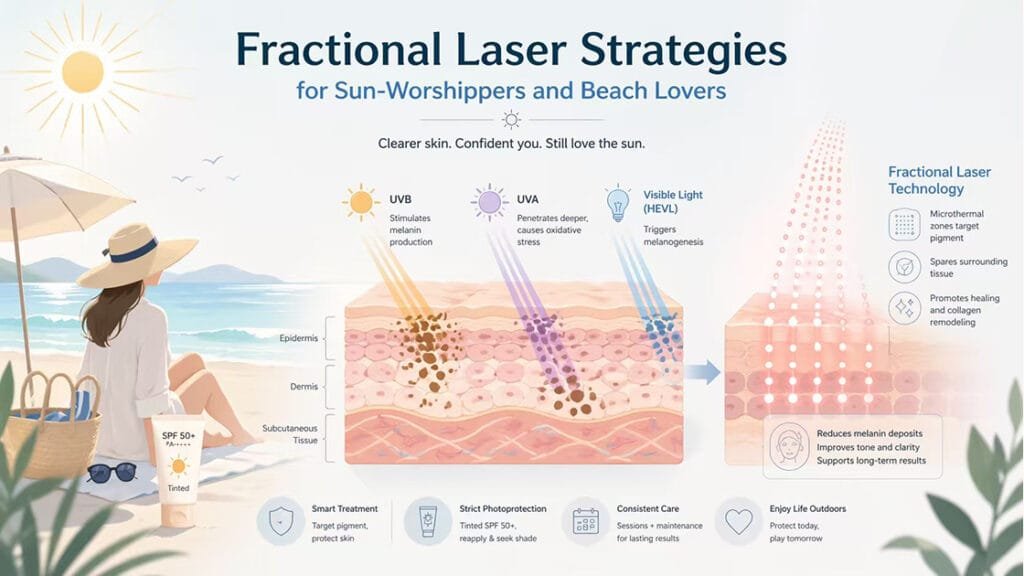
Ultraviolet radiation represents the single most significant environmental trigger for melasma. UVB stimulates keratinocytes to produce α-MSH, leading to melanocyte proliferation and increased melanin synthesis. UVA penetrates deeper into the dermis, causing oxidative stress and immediate pigment darkening. UV light also induces reactive oxygen species, and melasma patients consistently demonstrate higher markers of oxidative stress.
1.3 Beyond UV: Hormones, Genetics, and Visible Light
Hormonal fluctuations during pregnancy, oral contraceptive use, and hormone replacement therapy can all initiate or exacerbate melasma. Genetic predisposition plays a significant role, with higher prevalence among individuals of Latin American, Asian, and Middle Eastern descent. Recent research has identified visible light (VL) as an additional contributor to melanogenesis, explaining why some patients develop pigmentation even when using traditional UV-blocking sunscreens.
2. The Treatment Challenge: Why Melasma Keeps Coming Back
2.1 The Recurrence Problem
Melasma follows a relapsing-remitting pattern, with pigmentation darkening during summer months or after UV exposure and lightening during winter or strict photoprotection. This chronic nature means that even after successful treatment, patients must remain vigilant about maintenance strategies indefinitely. Traditional approaches relying solely on topical bleaching agents often yield disappointing long-term results.
2.2 Limitations of Topical Therapies Alone
First-line topical treatments include hydroquinone, tretinoin, corticosteroids, kojic acid, and azelaic acid. Their effects typically plateau after several months, and prolonged use carries risks of irritation, contact dermatitis, and ochronosis. Importantly, topical therapies primarily target epidermal melanin and have limited penetration into the dermis. This explains why many patients experience incomplete clearance or rapid recurrence.
2.3 Why Laser Therapy Must Be Approached with Caution
Not all laser treatments work well for melasma. Aggressive laser approaches can worsen the condition by triggering post-inflammatory hyperpigmentation, especially in darker skin phototypes. Traditional ablative lasers carry high risks for both hyperpigmentation and hypopigmentation. The key lies in selecting technologies that selectively target melanin while minimizing thermal damage to surrounding tissues.
3. How Fractional Laser Technology Works for Melasma
3.1 The Principle of Fractional Photothermolysis
Fractional laser technology creates microscopic columns of thermal injury—microthermal zones—while leaving surrounding tissue intact. These columns extend to controlled depths depending on wavelength and energy settings. The intact bridges of healthy skin serve as reservoirs for rapid re-epithelialization, typically completing within 24 hours, and provide stem cells and growth factors that accelerate healing.
3.2 Targeting Melanin While Sparing Surrounding Tissue
The mechanism involves selective photothermolysis of melanin-rich structures. Laser energy at specific wavelengths is preferentially absorbed by melanin, causing targeted destruction of hyperactive melanocytes and fragmentation of existing pigment granules. This process, sometimes called laser toning, reduces both epidermal and dermal melanin deposits without causing widespread thermal injury.
3.3 Non-Ablative vs. Ablative Fractional Lasers
Non-ablative fractional lasers (NAFLs) create thermal injury without vaporizing tissue, preserving the stratum corneum and reducing downtime. Strong evidence supports NAFL treatment for melasma across skin types III-VI. Ablative fractional lasers vaporize tissue and penetrate more deeply, carrying higher risks of post-inflammatory pigmentation. Many clinicians reserve ablative approaches for carefully selected patients.
4. Clinical Principles of Fractional Laser Treatment
4.1 Parameter Selection and Individualization
Successful melasma treatment with fractional lasers depends heavily on precise energy density, coverage density, and pulse count. Excessive energy can trigger post-inflammatory hyperpigmentation, while insufficient energy yields poor results. Clinicians must individualize parameters based on the patient‘s skin phototype, pigment depth, and prior treatment response. A low-energy, multiple-session strategy generally provides safe cumulative benefits.
4.2 The Need for Combination Therapy
Fractional laser alone rarely achieves long-term melasma control. Clinical consensus supports laser therapy as part of a comprehensive management plan, not a standalone tool. After laser disrupts pigment granules, combining it with topical depigmenting agents suppresses residual melanocyte activity. Oral antifibrinolytic agents may reduce melanin formation systemically. This multi-target synergy significantly improves success rates and durability.
4.3 Treatment Intervals and Course Design
Melasma responds slowly to laser treatment, requiring adequate intervals for skin repair and visible improvement. Typical protocols recommend one session every 4‑6 weeks, with a full course of 4‑6 treatments. Excessive session frequency increases irritation risk, while overly long intervals allow pigment rebound. After the initial course, most patients need maintenance every 3‑4 months to counter seasonal and environmental triggers.
4.4 Prevention and Management of Adverse Effects
Although fractional lasers are relatively safe, clinicians must remain vigilant for pigmentary complications. Pre‑treatment assessment of post-inflammatory hyperpigmentation risk is essential. Darker skin phototypes require lower energy settings and longer intervals. Immediate post‑treatment cooling reduces thermal injury, while strict sun protection and antioxidant use lower pigmentation risk. If pigmentation darkens, laser treatment should pause while anti‑inflammatory and depigmenting therapy begins.
5. The Non-Negotiable Role of Photoprotection
5.1 Beyond Traditional Sunscreen: Visible Light Protection
Standard sunscreens that block only UV radiation prove insufficient for melasma patients. Visible light, particularly high-energy visible light in the blue-violet spectrum, stimulates melanogenesis independently. Tinted sunscreens containing iron oxides reduce HEVL transmission by up to 80% to 97% and improve clinical outcomes. These formulations should replace non-tinted sunscreens for hyperpigmentation-prone patients.
5.2 Daily Habits for Beach Lovers and When to See a Specialist
Patients need not abandon outdoor passions but must adopt rigorous habits: apply SPF 50+ sunscreen daily, reapply every two hours at the beach, wear wide-brimmed hats and UV-protective clothing, and seek shade from 10 a.m. to 4 p.m. Those with active skin infections, pregnancy, keloid history, or inability to commit to daily photoprotection may not be ideal candidates. Always consult a board-certified dermatologist with melasma expertise.
FAQ
Q: Can I ever go back to the beach after treating my melasma?
A: Yes, but you must commit to strict photoprotection. Use tinted mineral sunscreen (SPF 50+), wear a wide-brimmed hat, and seek shade during peak hours.
Q: How many fractional laser sessions will I need?
A: Most patients require four to six sessions spaced 4‑6 weeks apart, followed by maintenance treatments every three to four months.
Q: Does fractional laser treatment hurt?
A: Most patients describe the sensation as mild pinpricks or rubber band snaps. Topical numbing cream makes the procedure comfortable for nearly everyone.
Q: Will my melasma come back after treatment?
A: Melasma is a chronic condition that can recur, especially with sun exposure. However, maintenance treatments and rigorous photoprotection can keep it under control long-term.
Q: Is fractional laser safe for darker skin types?
A: Yes, when performed by an experienced provider using appropriate non-ablative fractional laser parameters with a low-energy, multiple-session strategy.
Schlussfolgerung
Melasma presents a genuine dilemma for sun-worshippers and beach lovers, but fractional laser strategies offer a path forward that does not require abandoning outdoor passions entirely. By selectively targeting melanin deposits while preserving surrounding tissue, fractional laser technology reduces pigmentation and improves skin clarity. When combined with rigorous photoprotection—including tinted sunscreens that block visible light—and appropriate maintenance treatments, fractional laser therapy can help patients regain clear, even-toned skin while continuing to enjoy the outdoor activities they love.
References
Aref, S. A., et al. (2025). Fractional non ablative 675 nm diode laser versus low fluence high frequency Q-switched 1064 nm nd: YAG laser in the treatment of melasma: a comparative split face trial. PMC.
Kelechi, T. J., et al. (2018). Symptoms Associated With Chronic Venous Disease in Response to a Cooling Treatment Compared to Placebo. Journal of Wound, Ostomy and Continence Nursing, 45(4), 301–309.
https://pubmed.ncbi.nlm.nih.gov/29846278
Kim, J. H., et al. (2025). Fractional CO2 Laser 2-Mercaptonicotinoyl Glycine Drug Delivery for Melasma and Facial Hyperpigmentation. MDPI.
Lee, S. Y., et al. (2025). Comparative efficacy of chemical peels and laser treatments in melasma: a meta-analysis of randomized controlled trials. KoreaMed.
https://journals_beta.koreamed.org
Mourot, L., et al. (2007). Hyperbaric gaseous cryotherapy: effects on skin temperature and systemic vasoconstriction. Archives of Physical Medicine and Rehabilitation, 88(10), 1339–1343.
https://pubmed.ncbi.nlm.nih.gov/17908579
Rokhsar, C. K., et al. (2010). Treatment of melasma using fractional photothermolysis: a report of eight cases with long-term follow-up. JoVE.







